The Biomedical Model Has a Shelf Life
Papers reviewed: Johnson MI, Bonacaro A, Georgiadis E, Woodall J (2024). "Editorial: Non-biomedical perspectives on pain and its prevention and management." Frontiers in Pain Research, 5:1404074. // Johnson MI et al. (2024). "Editorial: Pain education research: advances, innovations, and challenges." Frontiers in Pain Research, 5:1403461. // Thompson K, Milligan J, Murphy A, Tabasam G, Johnson MI (2024). "'Unmasking Pain' through creativity: A phenomenological study of person-centred pain exploration for people living with chronic pain." PLOS ONE, 19(10):e0312014.
There is a question worth sitting with before your next client walks through the door: are you treating a tissue, or are you treating a person?
This isn't a rhetorical provocation. It is, increasingly, a clinical one — and a growing body of research is pointing massage therapists, physiotherapists, and most manual practitioners toward an uncomfortable answer. The biomedical model — the one most of us were trained in, the one that names muscles and grades inflammation and maps the dermatomes — is not wrong. But for a significant proportion of the people we see, it is no longer enough.
This model that built our profession - lets not throw it out!
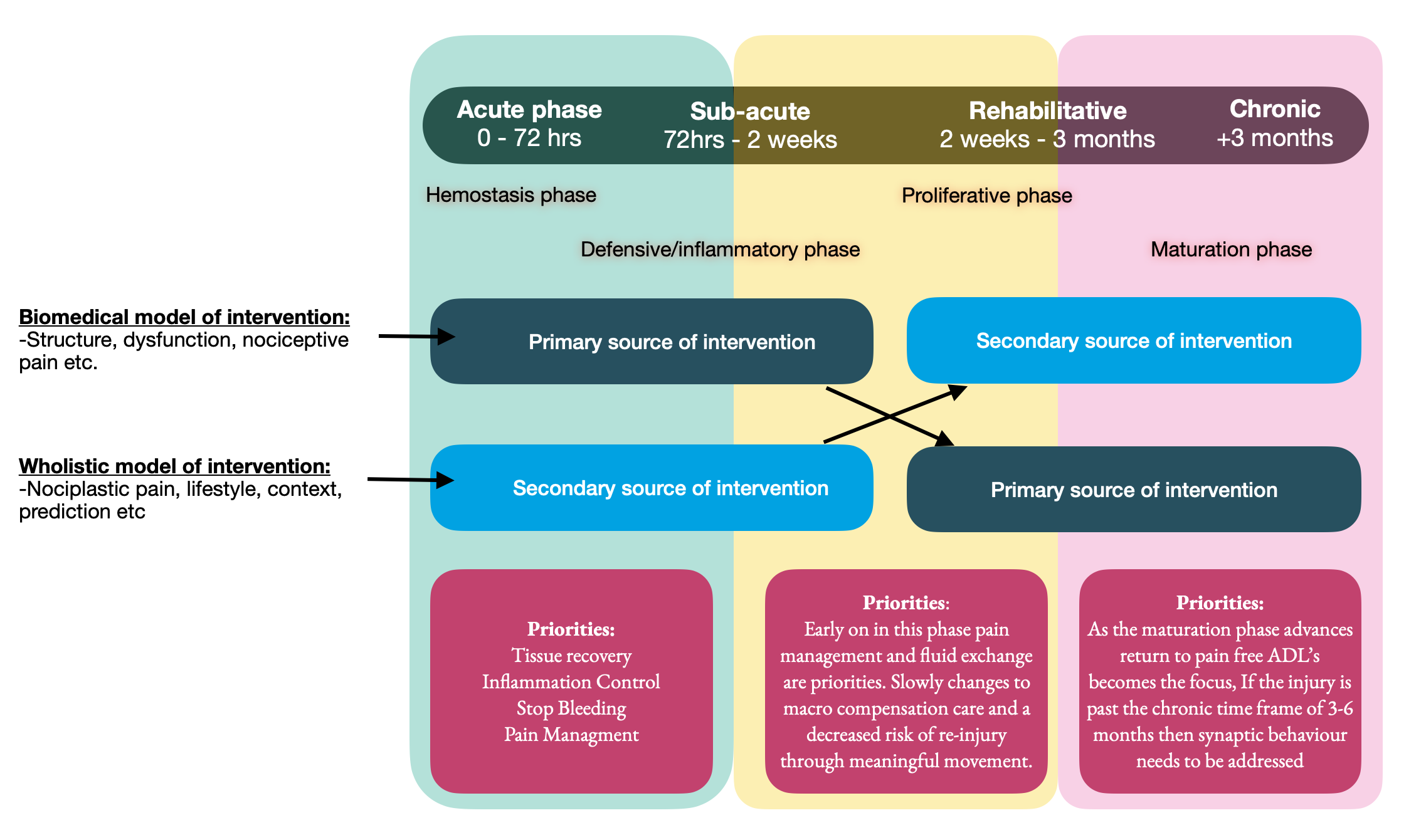
Credit where credit is due. Let's be fair to the biomedical paradigm first. It gave us anatomy, pathophysiology, tissue healing timelines, and the foundational language of clinical reasoning. When someone walks in three weeks post-ankle sprain, or five days after a minor disc bulge, the biomedical model is doing exactly what it was designed to do: tracking tissue damage and recovery timeframes. That framework belongs in the acute/sub-acute and rehabilitative phase — from day of injury to roughly three months — and it belongs there for good reason.
My question is what happens when the tissue has healed during or after that timeframe and the pain persists? What happens when imaging finds nothing, nerve conduction studies come back clean, and yet your client is still in agony six months later? Or possibly worse, what happens when imaging finds something but your client is asymptomatic? (I discuss this in my first blog post here) This is where the model starts to strain — and where some research being published in 2024 is asking us to think more carefully.
A recently published editorial collection in Frontiers in Pain Research, led by Johnson, Bonacaro, Georgiadis and Woodall, brings together seventeen articles — theoretical and empirical — from disciplines that rarely appear in a typical pain science curriculum. Anthropology. History. Ecology. Philosophy. The Arts. The editorial argues that overreliance on the biomedical paradigm has contributed, in part, to overuse of surgery and long-term drug medication with harmful physical, psychological, social, and economic consequences. Research has been dominated by a tissue-centric view of pain at the expense of the holistic, first-person experience of living with pain in community.
What strikes me about this framing is not that it dismisses structure. It is that it asks where we are looking when the tissue story runs out.
One of the most striking contributions in the collection of papers that it proposes a socio-ecological model of pain that situates the body inside a layered web of determinants: personal circumstances, social connections, working conditions, cultural narratives, even climate and built environment. Think of the layered web of determinants like Allostatic load (the cumulative "wear and tear" on the body and brain that results from chronic exposure to, or inefficient management of, repeated or prolonged stress). The model argues that viewing pain through an evolutionary mismatch lens can reveal upstream forces that create what the authors call "painogenic environments" — conditions that make pain more likely to develop and more difficult to resolve. The biomedical paradigm, these papers suggests, tends to act as a kind of social glue, reinforcing a narrative about pain that primes patients for passive treatment rather than active recovery. (Reflect on all the social media posts, billboards, ads on TV that promote the biomedical model of posturology, dysfunction movement patterns, sleep positions etc.)

Another thread in the collection concerns the language we use.
Drawing on philosophical work in linguistic relativity, one contribution makes the case that damage-loaded metaphors — "tearing," "grinding," "bone on bone" — may actually shape a patient's lived experience of their pain, reinforcing catastrophizing and making recovery more difficult. If we want people to move forward, the research argues, we may literally need to change the metaphors we offer.
This is where the pain education breaks down
A companion editorial in the same journal — this one on pain education — provides a useful parallel. Johnson and colleagues, writing with researchers from Tufts University School of Medicine and the University of Toronto, observe that worldwide consensus has identified pain education for health care professionals as inadequate to meet clinical need. A particular concern across multiple contributions in that collection is that medical curricula remain biophysically focused, with biopsychosocial approaches and interprofessional learning underrepresented — particularly in North American medical schools.
One contribution in the education research series describes what the authors call "didactic dissonance": a disconnect between what students are taught in classroom settings and what they observe in clinical environments. Another describes a hidden curriculum entrenched in the biomedical model — a set of values and assumptions students absorb not from textbooks but from watching how their supervisors practice. Both paint a picture of a system that is aware it needs to change but is finding the change genuinely difficult.
For massage therapists, this matters because we are embedded in that same ecosystem. Our referrals come from that system, our language often mirrors it, and our clients arrive carrying its narratives about what their pain means.
I propose that a possible solution is the intermingling of professional development requirements amongst practitioners from varying disciplines. If massage therapists begin attending courses that are offered by physiotherapist, chiropractors and vis-versa, the sharing of knowledge and interchanging of focus and concentration is likely to enhance a more person centered approach and transition away from a tissue centric modalities.
Thinking beyond the clinic space
Perhaps the most quietly remarkable paper in this group is a phenomenological study published in PLOS ONE by Thompson, Milligan, Murphy, Tabasam, and Johnson. It documents the lived experience of people with chronic pain who participated in something called the Unmasking Pain project — an artist-led initiative funded by Arts Council England that brought together people living with fibromyalgia, Parkinson's, arthritis, and other persistent pain conditions for creative workshops involving dance, clay work, puppetry, and art.
What the researchers found is worth pausing on. Three overarching themes emerged from participant interviews. The first — Space to Breathe — describes an environment of dissolved hierarchy and genuine human connection, explicitly contrasted with clinical encounters. The second — Flexibility to Participate — describes the experience of engaging on one's own terms, without pressure, without a predetermined endpoint. The third — Possibility for Change — documents something the participants hadn't expected: a reforming of their relationship to pain, a liberation in the moment, and a renewed orientation toward the future.
This was not therapy. The artists were not clinicians. There was no treatment goal. And yet participant after participant described their pain experience as transformed — not eliminated, but reframed, externalised, given new form. One described it as having a new set of rules. Another said it simply gave them hope to carry on.
The study's authors are careful to note the limitations of a small qualitative sample. But they are also clear about the implication: arts-based, community-led, non-clinical approaches may offer something that clinical pathways currently cannot, particularly for people who have been living with pain for years.
How does the change what YOU do?
None of this is an argument against structural assessment. The thoracic hypomobility, the hypertonic piriformis, the compensatory scapular pattern — these are real, and addressing them matters, especially in the early weeks/months of an injury. In the acute, subacute-rehabilitative window, the biomedical model is our primary language and it should be. (This also happens to be where a lot of massage therapy education remains both at the baseline educational level as well in professional development.)
But when a client has been in pain for four, six, twelve months — when they have seen three practitioners, tried two imaging protocols, and still can't sleep — the tissue story is no longer the whole story. At that point, the research is telling us that the questions worth asking look different. What is their life like? What do they believe about their pain? What do they feel they can no longer do — and have they been given space to grieve that? Who do they talk to about it? What gives them meaning? (This may mean finding a talk therapist to refer out to.)
This is the territory I explore in Pain: The Other 4-Letter Word— the idea that chronic pain is not simply a biological signal gone rogue, but a deeply human experience shaped by psychology, relationships, environment, and narrative. The research reviewed here is not a departure from that framework. It is the academic literature catching up to it.
To be clear this is a shift in perspective, not a rejection of structure
What the Johnson et al. collection ultimately advocates for is not the abandonment of biomedicine. It is the development of what the authors call an ecology of pain — a richer, more layered understanding of why pain persists in the complex sociological milieu of modern life, and what genuinely helps people live well within it.
For those of us working with our hands, that means holding two things at once. A sophisticated understanding of tissue, movement, and neurophysiology — applied rigorously in the early stages of injury. And, as injuries move into the chronic phase, a willingness to shift the frame: to ask about the person, not just the structure; to use language that opens possibility rather than reinforcing damage; and to see the therapeutic relationship itself as one of the most powerful tools in the room.
The research is not asking us to stop being body workers. It is asking us to remember that the body we are working with is inhabited by a person — and that person lives in a world.